Certificate of Need Reform: Answering the Fears

A certificate of need (CON) is a government-mandated permission slip to open or expand healthcare facilities. Without a CON, providers in states with CON laws cannot open a new healthcare facility or offer new or expanded services at an existing healthcare facility. An applicant seeking a CON must prove to the government’s satisfaction that the public needs the applicant’s services. Furthermore, in most states with CON laws, incumbent providers can participate in the application process to keep new competition from entering the market, leaving fewer healthcare choices for patients.
The original intent behind CON laws was to lower healthcare spending and to increase quality and accessibility. In 1974, Congress enacted the National Health Planning and Resources Development Act (NHPRDA) to reduce federal healthcare spending.1Pub. L. No. 93-641, 88 Stat. 2225 (1975), repealed by Pub. L. No. 99-660, § 701, 100 Stat. 3743, 3799 (1986). NHPRDA conditioned certain federal healthcare reimbursements for states on the adoption of CON laws. At one point, every state except Louisiana had adopted a CON program.2Louisiana later adopted a CON program, which it calls facility need review (FNR). Louisiana continues to enforce FNR today.
In 1986, Congress repealed NHPRDA, recognizing that CON laws had been an abject failure. Members of Congress supporting CON law repeal remarked that CON laws “failed to control healthcare costs and [were] insensitive to community needs.”3Patrick John McGinley, “Beyond Health Care Reform: Reconsidering Certificate of Need Laws in A ‘Managed Competition’ System,” Florida State University Law Review 23, no. 1 (1995): 157; US Department of Health and Human Services, US Department of the Treasury, and US Department of Labor, Reforming America’s Healthcare System through Choice and Competition, December 3, 2018, 50 (recommending repeal or significant reduction of CON laws). Since that time, every presidential administration, both Democratic and Republican, has called on states to repeal their CON laws because they fail to decrease costs or increase quality and access.
Many states have repealed or scaled back their CON laws.4For example, in 2023, South Carolina repealed all its CON laws except for those governing nursing homes (S.B. 164, 125th Sess. (S.C. 2023)). Tennessee enacted major reforms in 2021 and 2024 (S.B. 672, 113th Gen. Assemb. (Tenn. 2023); H.B. 2269 113th Gen. Assemb. (Tenn. 2024)). In 2025, the District of Columbia enacted reforms (72 D.C. Reg. 6762 (Jun. 20, 2025)), and Wyoming repealed its lone remaining CON law (for nursing homes) (H.B. 289, 68th Leg., 2025 Gen. Sess. (Wyo. 2025)). As a result, 40 percent of the nation’s population lives in a state with no CON laws or few CON laws (see Figure 1), which allows academics to compare outcomes between CON-law states and non-CON-law states. In fact, this has become one of the most well-studied areas of policy.
Figure 1. States with Three or More Healthcare CONs
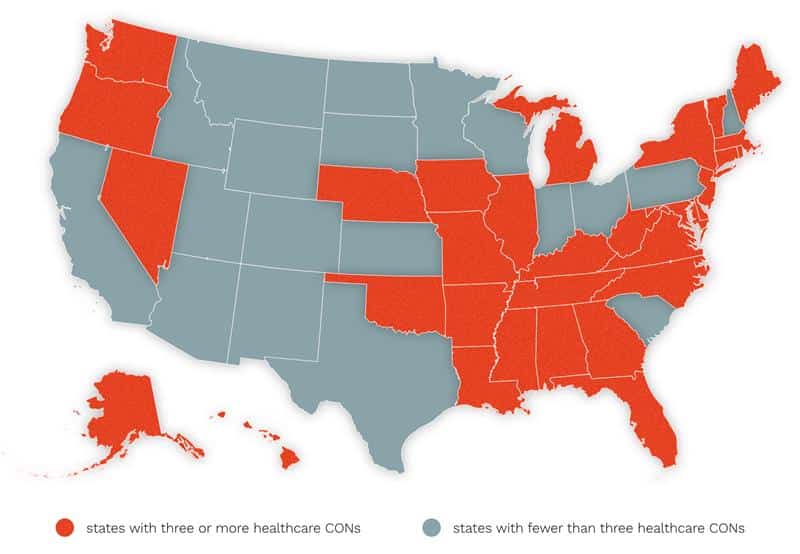
Source: Authors’ assessment based on survey of statutes and CON programs.
Other states have been enforcing CON laws since the 1960s or 1970s without any meaningful reforms. These states have been artificially suppressing the growth of healthcare facilities and services for decades, which could leave residents underserved as they age and miss out on advancements in technology and greater availability of healthcare. Table 1 lists several services and technologies and the numbers of states that require a CON for each.
Table 1. Services and Technologies for Which States Require a CON
| Service or Technology | Number of States That Require a CON for the Service or Technology |
|---|---|
| Nursing Home Beds and Long-Term Care Beds | 34 |
| Psychiatric Services | 31 |
| New Hospitals or Hospital-Sized Investments | 29 |
| Intermediate Care Facilities for Individuals with Intellectual Disabilities | 28 |
| Hospital Beds (e.g., Acute, General, Medical-Surgical) | 27 |
| Long-Term Acute Care | 25 |
| Ambulatory Surgical Centers (ASC) | 24 |
| Cardiac Catheterization | 24 |
| Rehabilitation | 24 |
| Substance or Drug Abuse | 24 |
| Open-Heart Surgery | 22 |
| Radiation Therapy | 21 |
| Magnetic Resonance Imaging (MRI) Scanners | 20 |
| Positron Emission Tomography (PET) Scanners | 19 |
| Neonatal Intensive Care | 18 |
| Organ Transplants | 18 |
| Home Health | 17 |
| Obstetrics Services | 16 |
| Hospice | 15 |
| Computed Tomography (CT) Scanners | 15 |
| Linear Accelerator Radiology | 15 |
| Mobile Hi Technology (e.g., CT, /MRI, /PET, etc.) | 15 |
| Renal Failure and Dialysis | 13 |
| Burn Care | 10 |
| Swing Beds | 10 |
| Assisted Living and Residential Care Facilities | 10 |
| Gamma Knives | 8 |
| Lithotripsy | 8 |
| Ground Ambulance | 8 |
| Air Ambulance | 6 |
| Ultrasound | 2 |
| Subacute Services | 1 |
Source: Matthew D. Mitchell and Stephen Slivinski, “After CON: What Happens When States Repeal or Modify Their Certificate of Need Requirements in Health Care?,” George Mason Law Review, accepted March 4, 2025, forthcoming.
Just as the types of facilities and services that require a CON vary by state, so too does the breadth of CON laws. Some states, such as Maine and West Virginia, restrict access to healthcare in more than a dozen categories, while other states, such as Indiana and Ohio, apply CON laws only to long-term care beds and facilities.5For an overview of each state’s CON laws as of 2020, see Jaimie Cavanaugh et al., Conning the Competition: A Nationwide Survey of Certificate of Need Laws (Arlington, VA: Institute for Justice, 2020).
This research in brief relies on the large body of academic research to dispel common myths about CON laws and their effects. In 2024, one of the authors (Matthew D. Mitchell) published a paper reviewing hundreds of academic tests of CON laws.6Matthew D. Mitchell, “Certificate-of-Need Laws in Healthcare: A Comprehensive Review of the Literature,” Southern Economic Journal 91, no. 1 (2025): 6–43. The results of those tests overwhelmingly show that CON laws fail to deliver on their promises of lower costs, increased access, and improved healthcare quality. Moreover, these tests show that when CON laws are repealed or relaxed, the doomsday scenarios predicted by supporters of CON laws simply do not play out in the real world.
These scenarios nevertheless dominate public discussion of CON reform, so this research in brief is organized around them. Ultimately, healthcare policy advocates, legislators, and healthcare providers should rely on real-world data, not speculation and fear.
Answering the Fears
As researchers who have studied and written about CON regulations for more than a decade, we are frequently invited to testify before legislative committees contemplating CON reform or repeal. Collectively, we have testified on CON laws more than 40 times. Although every hearing is a little different, they have common themes. One is that industry insiders, especially hospital associations, are reliably opposed to the elimination or relaxation of CON laws.
Their incentives for opposition are obvious enough. As a regulatory barrier to entry, CON laws limit their competition. Standard economic theory suggests that such a barrier will tend to permit incumbent providers to capture a larger share of the market and to earn above-normal profits known to economists as “rent.” In other words, in supporting CON laws, industry insiders behave just as economic theory predicts they would.7George J. Stigler, “The Theory of Economic Regulation,” Bell Journal of Economics and Management Science 2, no. 1 (1971): 3–21; Gordon Tullock, “The Welfare Costs of Tariffs, Monopolies, and Theft,” Western Economic Journal [Economic Inquiry] 5, no. 3 (1967): 224–32; Ernesto Dal Bó, “Regulatory Capture: A Review,” Oxford Review of Economic Policy 22, no. 2 (2006): 203–25.
Special interests, however, are unlikely to win a case that rests entirely on personal gain. Instead, they typically argue that the regulation serves the public interest. To that end, they tend to make five main arguments.
Fear 1: Without CON Laws, Costs Will Rise as Hospitals Acquire Expensive and Unnecessary Equipment
This argument is one of the original rationales for CON. Indeed, the opening pages of NHPRDA lament the “massive infusion of Federal funds into the existing heath care system [that] has contributed to inflationary increases in the cost of health care.”8National Health Planning and Resources Development Act of 1974, Pub. L. No. 93-641, 88 Stat. 2225 (1975). Then, as now, many people attributed the high cost of American healthcare to information asymmetry and the third-party payer problem. Because patients are not as informed as their providers and because they are rarely paying the full marginal cost of their care, a provider with an expensive service to sell can often convince patients to obtain the service regardless of whether they need it.
To bolster their case, the advocates of CON often point to a 1959 study coauthored by UCLA health researcher Milton Roemer.9M. Shain and Milton I. Roemer, “Hospital Costs Relate to the Supply of Beds,” Modern Hospital 92, no. 4 (1959): 71–73. Roemer and his coauthor find a positive correlation between the number of hospital beds available per capita and the number of used hospital days per capita. The finding, often shortened into the maxim that “in an insured population, a hospital bed built is a hospital bed filled” has become known as Roemer’s Law.10University of California, Los Angeles, “Obituary: Milton I. Roemer, Pioneering UCLA Health Services Professor and Professional Who Defined Health Policy in U.S., Abroad,” press release, January 8, 2001, https://web.archive.org/web /20120304021055/http://www.ph.ucla.edu/pr/miroemer.html.
By limiting the number of beds (and hospitals, dialysis clinics, psychiatric care facilities, etc.), the advocates of CON contend that the regulation will save payors money. After all, if there are no available beds or psychiatric care facilities, there is no way to spend money on them.
There are two main problems with this argument. First, by limiting supply and reducing competition, CON is likely to increase the amount spent per service rendered. As economists Jon Ford and David Kasserman explained three decades ago, “the economic effect [of CON laws] is to shift the supply curve of the affected service back to the left,” and “the effect of such supply shifts is to raise . . . [the] equilibrium price.”11Jon M. Ford and David L. Kaserman, “Certificate-of-Need Regulation and Entry: Evidence from the Dialysis Industry,” Southern Economic Journal 59, no. 4 (1993): 783–91.
Even if CON succeeds in encouraging people to consume fewer healthcare services, that success is offset by peoples’ spending more for the services they do consume. In fact, since the demand for healthcare services is relatively insensitive to changes in price (i.e., demand is inelastic), the price-increasing effects of CON are likely to outweigh the quantity-reducing effects of CON.12Matthew D. Mitchell, “Do Certificate-of-Need Laws Limit Spending?” (Mercatus Working Paper, Mercatus Center at George Mason University, Arlington, VA, September 2016); James Bailey, “Can Health Spending Be Reined In through Supply Constraints? An Evaluation of Certificate-of-Need Laws” (Mercatus Working Paper Mercatus Center at George Mason University, Arlington, VA, August 1, 2016); James Bailey, “Can Health Spending Be Reined in through Supply Restraints? An Evaluation of Certificate-of-Need Laws,” Journal of Public Health 27, no. 6 (2019): 755–60; James Bailey and Tom Hamami, “Competition and Health-Care Spending: Theory and Application to Certificate of Need Laws” (working paper no. 19-38, Federal Reserve Bank of Philadelphia, Philadelphia, PA, October 2019).
The second problem with this argument is that it is not clear that reducing healthcare spending by rationing care is a worthwhile goal. Healthcare is not a bad like pollution or garbage; it is a good that people desire. An extremely stringent CON program could reduce spending to zero by eliminating all healthcare services, but consumer welfare would clearly be harmed by such a measure.
Although some healthcare procedures are unwarranted—a patient may not be a good candidate for a hip replacement, or a CT scan may produce a better (and cheaper) image than an MRI if a patient has metal implants—local providers, not distant regulators, possess the local knowledge to make these sorts of evaluations. Moreover, these tradeoffs should be made on a case-by-case basis, not at a community or state level.
To the extent that the third-party payer problem encourages unwarranted procedures, the best way to deal with this problem is to reform the policies that divorce consumers from cost.13John H. Cochrane, “After the ACA: Freeing the Market for Healthcare,” in The Future of Healthcare Reform in the United States, ed. Anup Malani and Michael H. Schill (Chicago, IL: University of Chicago Press, 2015), 161–201. By contrast, CON regulations restrict the ability of everybody—including customers who pay out of pocket—to access healthcare services.
The evidence bears this out. Several comparisons between states with and without CON laws are possible. One comparison is spending per service. To date, economists and healthcare researchers have conducted 45 separate evaluations of this question, comparing spending per service in CON-law and non-CON-law settings (see Figure 2). Of those tests, 60 percent find an association between CON laws and greater spending per service, whereas only 7 percent of tests find an association between CON laws and less spending per service.
Figure 2. Tests Assessing the Effects of CON Laws on Spending per Service
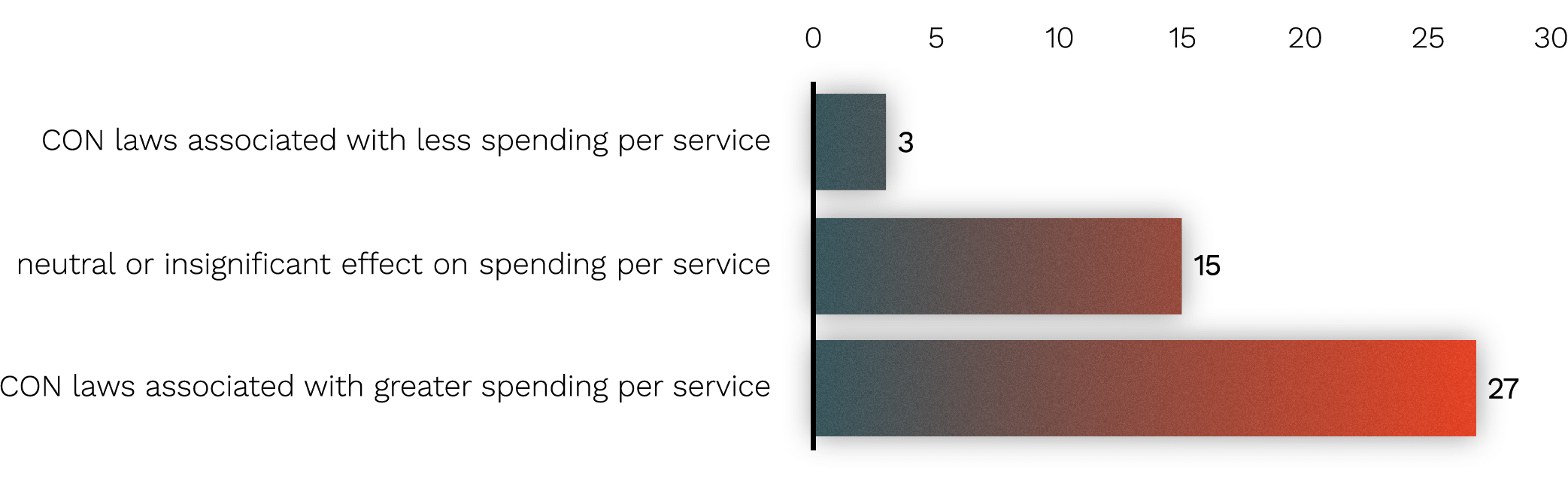
Source: Matthew D. Mitchell, “Certificate-of-Need Laws in Healthcare: A Comprehensive Review of the Literature,” Southern Economic Journal 91, no. 1 (2025): 6–43, updated to account for more recent publications.
Another comparison is spending per person (i.e., per patient). Fifty-two empirical tests have taken this approach (see Figure 3). The evidence shows that CON laws are associated with, if anything, more spending per person, not less.
Figure 3. Tests Assessing the Effects of CON Laws on Spending per Capita
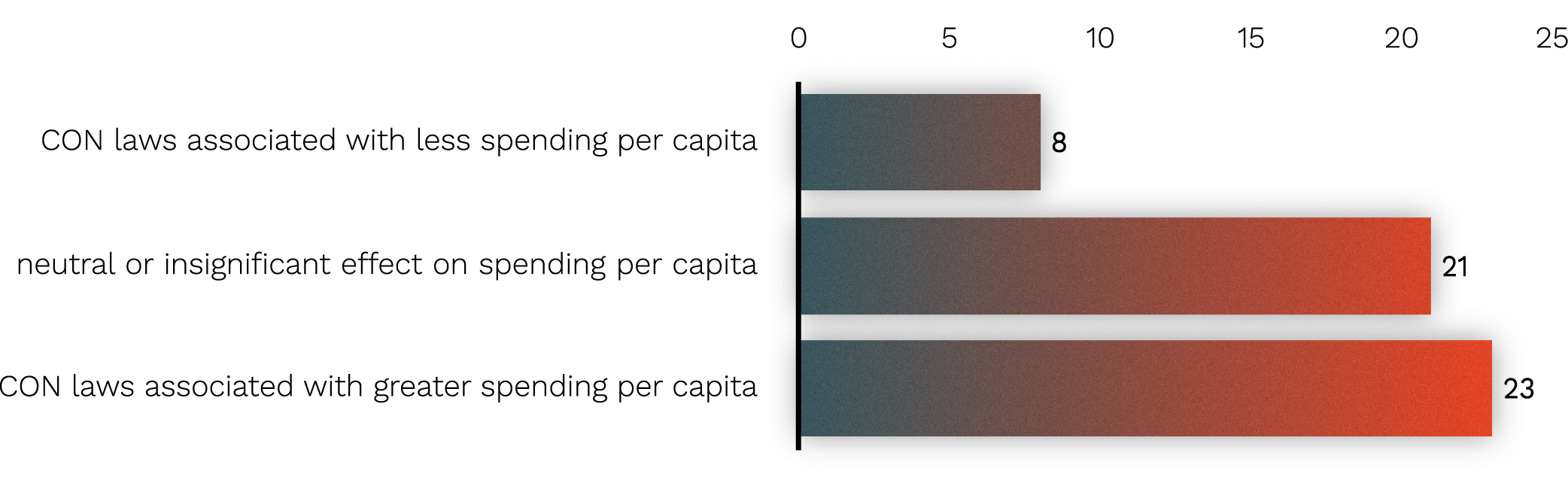
Source: Matthew D. Mitchell, “Certificate-of-Need Laws in Healthcare: A Comprehensive Review of the Literature,” Southern Economic Journal 91, no. 1 (2025): 6–43, updated to account for more recent publications.
Fear 2: Without CON, Hospitals—Especially in Rural Areas—Will Disappear
On its face, this is a counterintuitive argument. CON laws are used to limit the number of healthcare facilities, so one would expect to see fewer hospitals and fewer rural hospitals in states with CON laws. And, in fact, the evidence confirms common sense.
There are more hospitals per capita in states that have repealed their CON laws. One study estimates that states with CON laws have 30 percent fewer hospitals per 100,000 residents.14Thomas Stratmann and Christopher Koopman, “Entry Regulation and Rural Health Care: Certificate-of-Need Laws, Ambulatory Surgical Centers, and Community” (Mercatus Working Paper, Mercatus Center at George Mason University, Arlington, VA, February 2016). Another finds an association between CON laws and 48 percent fewer hospitals per capita and 12 percent fewer hospital beds per capita.15Traci L. Eichmann and Rexford E. Santerre, “Do Hospital Chief Executive Officers Extract Rents from Certificate of Need Laws?,” Journal of Health Care Finance 37, no. 4 (2011): 1–14. When researchers isolate rural areas, they find that states with CON laws have 30 percent fewer rural hospitals and 13 percent fewer rural ambulatory surgical centers (ASCs).16Stratmann and Koopman, “Entry Regulation and Rural Health Care.” Thus, evidence shows that when states repeal CON laws, more hospitals open, and they stay open. This evidence should end the debate.
The fact that states with CON laws have fewer facilities has real consequences. During the COVID-19 pandemic, hospitals in states with CON laws were 27 percent more likely to run out of beds.17Matthew D. Mitchell and Thomas Stratmann, “The Economics of a Bed Shortage: Certificate-of-Need Regulation and Hospital Bed Utilization during the COVID-19 Pandemic,” Journal of Risk and Financial Management 15, no. 1 (2022): 10. This pattern extends beyond hospitals. States with CON laws have 20 percent fewer psychiatric care facilities,18James Bailey and Eleanor Lewin, “Certificate of Need and Inpatient Psychiatric Services,” Journal of Mental Health Policy and Economics 24, no. 4 (2022): 117–124. fewer medical imaging devices,19Thomas Stratmann and Jacob W. Russ, “Do Certificate-of- Need Laws Increase Indigent Care?” (working paper no. 14-20, Mercatus Center at George Mason University, Arlington, VA, July 2014). and fewer open-heart surgery programs.20J. L. Robinson et al., “Certificate of Need and the Quality of Cardiac Surgery,” American Journal of Medical Quality 16, no. 5 (2001): 155–160.
Finally, one 2024 study finds that following the repeal of CON laws for ASCs, rural areas saw increases of 92 percent to 112 percent in ASCs per capita,21Thomas Stratmann, Markus Bjoerkheim, and Christopher Koopman, “The Causal Effect of Repealing Certificate‐of‐ Need Laws for Ambulatory Surgical Centers: Does Access to Medical Services Increase?,” Southern Economic Journal 92, no. 2 (2023): 1–24. greater increases than in urban areas. Notably, the authors find “no evidence that CON repeal is associated with hospital closures in rural areas. Rather, some regression models show that repeal is associated with fewer medical service reductions.”22Stratmann, Bjoerkheim, and Koopman, “The Causal Effect of Repealing,” 1.
Availability of services is one of the most studied aspects of CON laws. Eighty-nine empirical tests have compared the availability of services in CON-law and non-CON-law states. As shown in Figure 4, 79 percent of these tests find an association between CON laws and diminished access to care.
Figure 4. Tests Assessing the Effects of CON Laws on Availability of Services
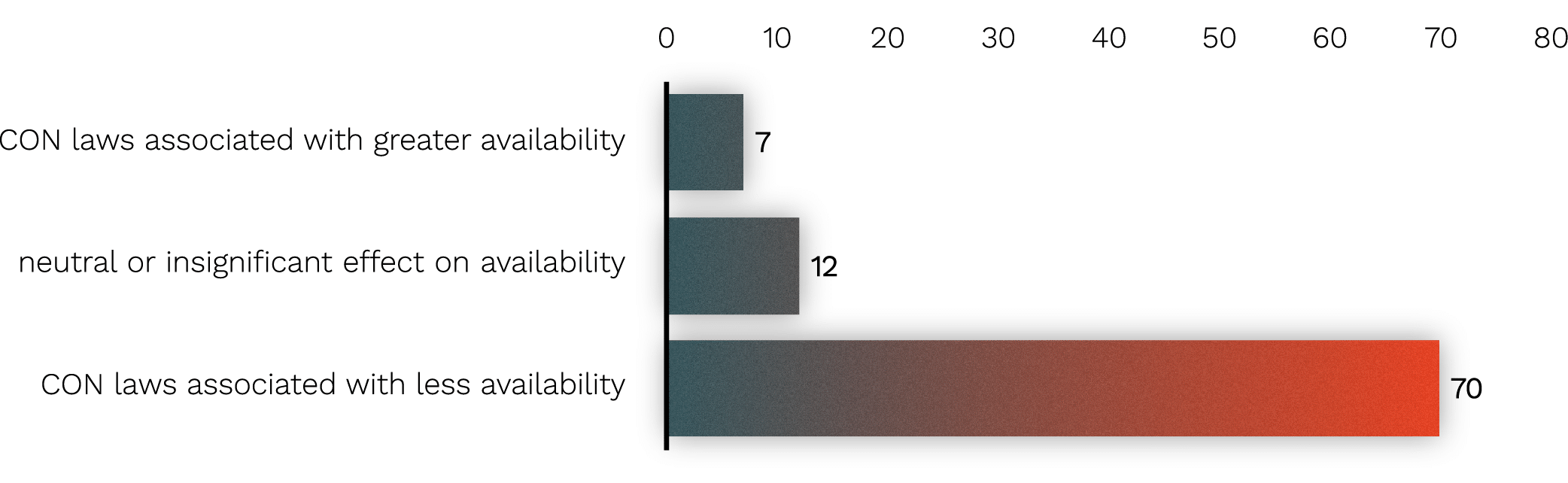
Source: Matthew D. Mitchell, “Certificate-of-Need Laws in Healthcare: A Comprehensive Review of the Literature,” Southern Economic Journal 91, no. 1 (2025): 6–43, updated to account for more recent publications.
Together, these studies debunk the myth that existing facilities close at a faster rate when states repeal CON laws, regardless of whether rural or urban areas are studied.
Several states with CON laws even make exceptions for rural areas, as if recognizing that CON laws are a barrier that prevent healthcare facilities from opening in the communities that often need care the most.23States with exceptions for CON laws in rural areas include Alabama (Ala. Code § 22-21-263), Kentucky (Ky. Rev. Stat. § 216B.020(3)(h), (l)), Maine (22 Me. Stat. § 330(7), Oregon (Or. Rev. Stat. §§ 442.315(8), .347), Tennessee (Tenn. Code § 68-11- 1626), and Washington (Wash. Admin. Code § 246-310-042(1)). These exceptions are a tacit admission that restricting the growth of healthcare facilities and services does not in fact create access to more healthcare.
Fear 3: Without CON Laws, ASCs Will Pop Up and Take Away All the Most Profitable Services from Hospitals
Despite the fact that more healthcare facilities open and remain open in states that have repealed their CON laws, proponents of CON laws continue to argue that if more ASCs or imaging facilities or birth centers are allowed to open, hospitals will close. The argument is attenuated, but proponents of CON laws claim that if privately insured patients start using new facilities instead of the hospitals, the hospitals’ margins will fall dramatically enough that they will be forced to discontinue services or close altogether. This is sometimes called “cream skimming” or “cherry picking” because incumbent hospitals fear that new providers will take the very best (highest paying) patients and procedures, leaving hospitals with less profitable lines of care. However, there is no evidence that hospitals close as a result of CON law repeal,24Stratmann, Bjoerkheim, and Koopman, “The Causal Effect of Repealing.” and this argument has several problems.
First, there is no reason to assume that all the privately insured patients will stop using hospitals. If hospitals offer high-quality, innovative care, they should not expect to see a mass exodus of patients.
Second, this argument assumes without evidence that every patient is already receiving the appropriate level of care and that hospitals will therefore lose some patients and that no new patients will seek care.
Third, economists have studied this issue and do not find evidence of “cream skimming” or “cherry picking.” Academics call this practice cost shifting, and the academic consensus is that cost shifting does not exist.25Austin B. Frakt, “How Much Do Hospitals Cost Shift? A Review of the Evidence,” Milbank Quarterly 89, no. 1 (2011): 90–130; Sherry Glied, “COVID-19 Overturned the Theory of Medical Cost Shifting by Hospitals,” JAMA Health Forum 2, no. 6 (2021): e212128. Hospitals argue that they rely on profits from commercially insured patients to make up for losses from underinsured or uninsured patients. If this were true, when Medicare or Medicaid lowers rates, one would expect to see costs for commercially insured patients rise to offset the supposed shortfall. On the contrary, the evidence shows that when government healthcare reimbursement rates go down, hospitals typically lower prices for commercially insured patients.26Jeffrey Clemens and Joshua D. Gottlieb, “In the Shadow of a Giant: Medicare’s Influence on Private Physician Payments,” Journal of Political Economy 125, no. 1 (2017): 1–39; Chapin White, “Contrary to Cost-Shift Theory, Lower Medicare Hospital Payment Rates for Inpatient Care Lead to Lower Private Payment Rates,” Health Affairs (Millwood) 32, no. 5 (2013): 935–43.
In 2020, the Congressional Budget Office examined this issue, concluding “the share of providers’ patients who are covered by Medicare and Medicaid is not related to higher prices paid by commercial insurers. That finding suggests that providers do not raise the prices they negotiate with commercial insurers to offset lower prices paid by government programs . . . .”27Congressional Budget Office, The Prices That Commercial Health Insurers and Medicaid Pay for Hospitals’ and Physicians’ Services, January 2022.
Likewise, the Colorado Department of Health Care Policy and Financing in 2020 investigated this issue and found, “this so-called need to shift costs to cover payment shortfalls is no longer a plausible or justifiable rationale for [hospital] price increases.”28Colorado Department of Health Care Policy and Financing, Colorado Hospital Cost Shift Analysis, January 2020.
Fourth, the premise that healthcare providers need monopoly control to stay afloat is directly contrary to the reason CON laws were first adopted—to restrain healthcare spending. Instead of arguing that CON laws have achieved this goal, healthcare providers implicitly argue that CON laws limit competition and ensure that patients have few choices for care, which allows healthcare providers to charge higher prices. And this, they argue, is a feature, not a bug.29The evidence is clear that CON laws increase healthcare prices and spending, which may be contributing to the medical debt crisis. See Noam N. Levey, “100 Million People in America Are Saddled with Health Care Debt,” KFF Health News, June 16, 2022.
Even if one were to accept as true that cost shifting was the only way to ensure the adequate availability of healthcare, research suggests CON laws do not aid in cost shifting. One study found that safety-net hospitals in states without CON laws had considerably higher margins than safety-net hospitals in states with CON laws.30Al Dobson et al., An Evaluation of Illinois’ Certificate of Need Program (Springfield, IL: State of Illinois Commission on Government Forecasting and Accountability, February 2007).
At this point, one might wonder why the cost-shifting myth has become so pervasive in healthcare policy debates. One Vermont CON regulator who studied this issue explains it as follows: The myth of the cost shift persist[s] . . . because it serves the interests of some very powerful forces in health care. First, it provides monopolistic hospitals and other profit-maximizing providers with a way to shift blame onto the government for their price gouging . . . . and remarkably, many state governments not only accept this lie but help enable it.31Thom Walsh, “Don’t Blame Medicare for Rising Medical Bills, Blame Monopolies,” Washington Monthly, June 19, 2023.
Fear 4: Without CON Laws, Quality Will Suffer Because CON Laws Lead to Fewer Providers, with Each Offering a Higher Volume of Care, and Higher Volume Leads to Greater Proficiency
As with some of the other arguments for CON laws, this one has an air of plausibility. It is well documented that providers who frequently perform a procedure tend to get better at it (though it is possible that causality could run in the opposite direction: especially competent providers may be in especially high demand), so if CON laws lead to fewer providers, and if those providers then perform more services, then it is plausible that CON laws will tend to improve the quality of care.
Though plausible, this argument must be weighed against two other plausible counterarguments. First, access to care is itself a dimension of quality, and CON clearly undermines this dimension. An expectant mother going into premature labor will likely be better served by a decent provider who is 15 minutes away than by a stellar provider who is an hour and a half away.32Economists sometimes refer to this as the “Cadillac effect” because it assumes that consumers will prefer no service at all if they can’t have the very best service at hand. Second, competition tends to improve quality, encouraging providers to offer the best outcomes and experiences they can or risk losing patients.
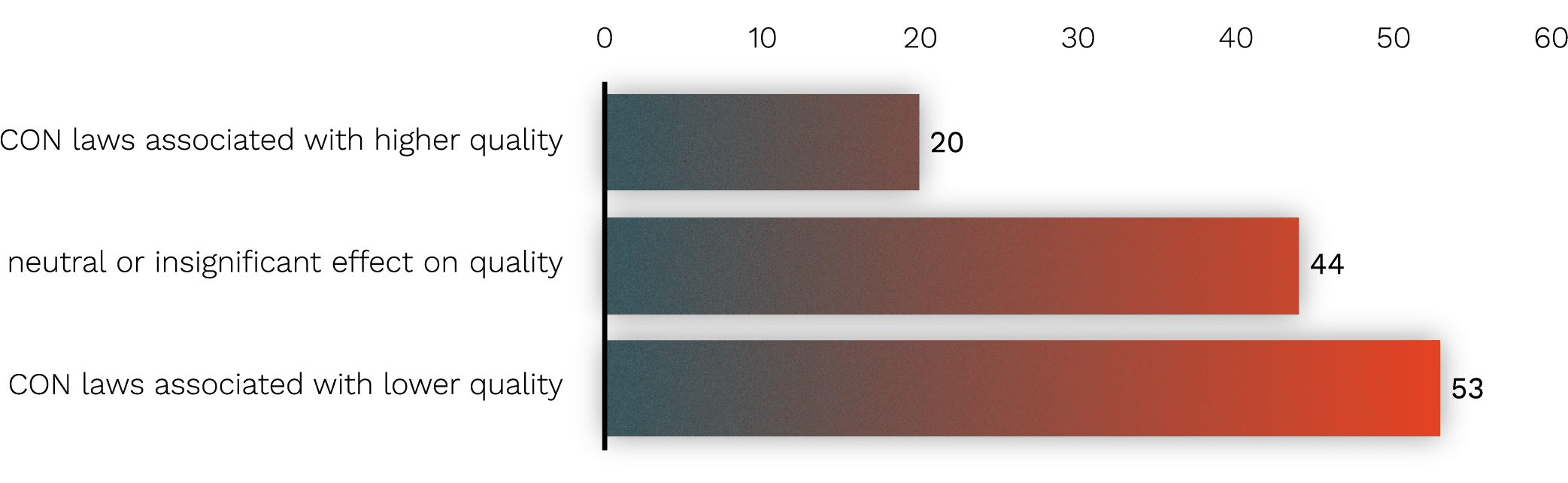
Again, the evidence bears out the counterarguments. To date, 113 tests have assessed the effect of CON laws on the quality of care that patients receive. Figure 5 summarizes these results. In 53 percent of these tests, CON laws are associated with lower quality of care. To take a few examples from this literature, one study finds that CON laws are associated with lower nursing staff-to-patient ratios and greater use of physical force in nursing homes.33J. S. Zinn, “Market Competition and the Quality of Nursing Home Care,” Journal of Health Politics, Policy and Law 19, no. 3 (1994): 555–82. Other studies find an association between CON and higher mortality rates following heart attack, heart failure, and pneumonia.34Thomas Stratmann, “The Effects of Certificate-of-Need Laws on the Quality of Hospital Medical Services,” Journal of Risk and Financial Management 15, no. 6 (2022): 272; Kevin Chiu, “The Impact of Certificate of Need Laws on Heart Attack Mortality: Evidence from County Borders,” Journal of Health Economics 79 (2021): 102518. Finally, one 2022 study finds that patients have higher mortality rates for natural death, septicemia, diabetes, chronic lower respiratory disease, influenza and pneumonia, Alzheimer’s disease, and COVID-19.35Agnitra Roy Choudhury, Sriparna Ghosh, and Alicia Plemmons, “Certificate of Need Laws and Health Care Use during the COVID-19 Pandemic,” Journal of Risk and Financial Management 15, no. 2 (2022): 76.
Figure 5. Tests Assessing the Effects of CON Laws on Quality of Care
Source: Matthew D. Mitchell, “Certificate-of-Need Laws in Healthcare: A Comprehensive Review of the Literature,” Southern Economic Journal 91, no. 1 (2025): 6–43, updated to account for more recent publications.
Fear 5: Healthcare Is Different: It Is Not a Free Market, So None of the Rules Apply
We conclude with the most enduring argument: healthcare is different. This argument can also be found in the NHPRDA, and it remains quite popular. It is often used as a retort to economists or others who note how absurd it would be if CON were applied in other markets—if, for example, McDonalds could object to a new Burger King.
It is true that there are plenty of problems with healthcare. The supply of providers is limited through scope-of-practice regulations; tax privileges and insurance mandates distort the market for insurance; and the third-party payer problem divorces consumers from the costs of the choices that they make. But in this case, another imperfection in the market does not correct for the others.
Even in healthcare, the standard rules of economics apply. Though healthcare markets are dominated by government payers, healthcare prices tend to be higher when there is less competition,36Zack Cooper et al., “The Price Ain’t Right? Hospital Prices and Health Spending on the Privately Insured” (NBER working paper no. 21815, National Bureau of Economic Research, Cambridge, MA, December 2015). which makes intuitive sense: providers can negotiate more favorable terms with insurers when they have fewer rivals. This fact explains why CON laws are associated with greater spending per service. Even in the unusual market of healthcare, a supply restriction tends to restrict the quantity supplied. This tendency also explains why CON laws are associated with fewer providers and less availability of services. And even in healthcare, more competition tends to correlate with higher quality, which explains why patients tend to experience better outcomes in non-CON-law than in CON-law states.
Conclusion
The elimination or relaxation of CON laws will not solve all that ails healthcare. However, based on the experiences of the 4 in 10 Americans who live in states with no or very limited CON regimes, it would appear to be a step in the right direction. Hundreds of tests confirm common sense: when supply is not limited by CON laws, patients have greater access to lower-cost and higher-quality care.
-
Sources
[1]
Pub. L. No. 93-641, 88 Stat. 2225 (1975), repealed by Pub. L. No. 99-660, § 701, 100 Stat. 3743, 3799 (1986).
[2]Louisiana later adopted a CON program, which it calls facility need review (FNR). Louisiana continues to enforce FNR today.
[3]Patrick John McGinley, “Beyond Health Care Reform: Reconsidering Certificate of Need Laws in A ‘Managed Competition’ System,” Florida State University Law Review 23, no. 1 (1995): 157; US Department of Health and Human Services, US Department of the Treasury, and US Department of Labor, Reforming America’s Healthcare System through Choice and Competition, December 3, 2018, 50 (recommending repeal or significant reduction of CON laws).
[4]For example, in 2023, South Carolina repealed all its CON laws except for those governing nursing homes (S.B. 164, 125th Sess. (S.C. 2023)). Tennessee enacted major reforms in 2021 and 2024 (S.B. 672, 113th Gen. Assemb. (Tenn. 2023); H.B. 2269 113th Gen. Assemb. (Tenn. 2024)). In 2025, the District of Columbia enacted reforms (72 D.C. Reg. 6762 (Jun. 20, 2025)), and Wyoming repealed its lone remaining CON law (for nursing homes) (H.B. 289, 68th Leg., 2025 Gen. Sess. (Wyo. 2025)).
[5]For an overview of each state’s CON laws as of 2020, see Jaimie Cavanaugh et al., Conning the Competition: A Nationwide Survey of Certificate of Need Laws (Arlington, VA: Institute for Justice, 2020).
[6]Matthew D. Mitchell, “Certificate-of-Need Laws in Healthcare: A Comprehensive Review of the Literature,” Southern Economic Journal 91, no. 1 (2025): 6–43.
[7]George J. Stigler, “The Theory of Economic Regulation,” Bell Journal of Economics and Management Science 2, no. 1 (1971): 3–21; Gordon Tullock, “The Welfare Costs of Tariffs, Monopolies, and Theft,” Western Economic Journal [Economic Inquiry] 5, no. 3 (1967): 224–32; Ernesto Dal Bó, “Regulatory Capture: A Review,” Oxford Review of Economic Policy 22, no. 2 (2006): 203–25.
[8]National Health Planning and Resources Development Act of 1974, Pub. L. No. 93-641, 88 Stat. 2225 (1975).
[9]M. Shain and Milton I. Roemer, “Hospital Costs Relate to the Supply of Beds,” Modern Hospital 92, no. 4 (1959): 71–73.
[10]University of California, Los Angeles, “Obituary: Milton I. Roemer, Pioneering UCLA Health Services Professor and Professional Who Defined Health Policy in U.S., Abroad,” press release, January 8, 2001, https://web.archive.org/web /20120304021055/http://www.ph.ucla.edu/pr/miroemer.html.
[11]Jon M. Ford and David L. Kaserman, “Certificate-of-Need Regulation and Entry: Evidence from the Dialysis Industry,” Southern Economic Journal 59, no. 4 (1993): 783–91.
[12]Matthew D. Mitchell, “Do Certificate-of-Need Laws Limit Spending?” (Mercatus Working Paper, Mercatus Center at George Mason University, Arlington, VA, September 2016); James Bailey, “Can Health Spending Be Reined In through Supply Constraints? An Evaluation of Certificate-of-Need Laws” (Mercatus Working Paper Mercatus Center at George Mason University, Arlington, VA, August 1, 2016); James Bailey, “Can Health Spending Be Reined in through Supply Restraints? An Evaluation of Certificate-of-Need Laws,” Journal of Public Health 27, no. 6 (2019): 755–60; James Bailey and Tom Hamami, “Competition and Health-Care Spending: Theory and Application to Certificate of Need Laws” (working paper no. 19-38, Federal Reserve Bank of Philadelphia, Philadelphia, PA, October 2019).
[13]John H. Cochrane, “After the ACA: Freeing the Market for Healthcare,” in The Future of Healthcare Reform in the United States, ed. Anup Malani and Michael H. Schill (Chicago, IL: University of Chicago Press, 2015), 161–201.
[14]Thomas Stratmann and Christopher Koopman, “Entry Regulation and Rural Health Care: Certificate-of-Need Laws, Ambulatory Surgical Centers, and Community” (Mercatus Working Paper, Mercatus Center at George Mason University, Arlington, VA, February 2016).
[15]Traci L. Eichmann and Rexford E. Santerre, “Do Hospital Chief Executive Officers Extract Rents from Certificate of Need Laws?,” Journal of Health Care Finance 37, no. 4 (2011): 1–14.
[16]Stratmann and Koopman, “Entry Regulation and Rural Health Care.”
[17]Matthew D. Mitchell and Thomas Stratmann, “The Economics of a Bed Shortage: Certificate-of-Need Regulation and Hospital Bed Utilization during the COVID-19 Pandemic,” Journal of Risk and Financial Management 15, no. 1 (2022): 10.
[18]James Bailey and Eleanor Lewin, “Certificate of Need and Inpatient Psychiatric Services,” Journal of Mental Health Policy and Economics 24, no. 4 (2022): 117–124.
[19]Thomas Stratmann and Jacob W. Russ, “Do Certificate-of- Need Laws Increase Indigent Care?” (working paper no. 14-20, Mercatus Center at George Mason University, Arlington, VA, July 2014).
[20]J. L. Robinson et al., “Certificate of Need and the Quality of Cardiac Surgery,” American Journal of Medical Quality 16, no. 5 (2001): 155–160.
[21]Thomas Stratmann, Markus Bjoerkheim, and Christopher Koopman, “The Causal Effect of Repealing Certificate‐of‐ Need Laws for Ambulatory Surgical Centers: Does Access to Medical Services Increase?,” Southern Economic Journal 92, no. 2 (2023): 1–24.
[22]Stratmann, Bjoerkheim, and Koopman, “The Causal Effect of Repealing,” 1.
[23]States with exceptions for CON laws in rural areas include Alabama (Ala. Code § 22-21-263), Kentucky (Ky. Rev. Stat. § 216B.020(3)(h), (l)), Maine (22 Me. Stat. § 330(7), Oregon (Or. Rev. Stat. §§ 442.315(8), .347), Tennessee (Tenn. Code § 68-11- 1626), and Washington (Wash. Admin. Code § 246-310-042(1)).
[24]Stratmann, Bjoerkheim, and Koopman, “The Causal Effect of Repealing.”
[25]Austin B. Frakt, “How Much Do Hospitals Cost Shift? A Review of the Evidence,” Milbank Quarterly 89, no. 1 (2011): 90–130; Sherry Glied, “COVID-19 Overturned the Theory of Medical Cost Shifting by Hospitals,” JAMA Health Forum 2, no. 6 (2021): e212128.
[26]Jeffrey Clemens and Joshua D. Gottlieb, “In the Shadow of a Giant: Medicare’s Influence on Private Physician Payments,” Journal of Political Economy 125, no. 1 (2017): 1–39; Chapin White, “Contrary to Cost-Shift Theory, Lower Medicare Hospital Payment Rates for Inpatient Care Lead to Lower Private Payment Rates,” Health Affairs (Millwood) 32, no. 5 (2013): 935–43.
[27]Congressional Budget Office, The Prices That Commercial Health Insurers and Medicaid Pay for Hospitals’ and Physicians’ Services, January 2022.
[28]Colorado Department of Health Care Policy and Financing, Colorado Hospital Cost Shift Analysis, January 2020.
[29]The evidence is clear that CON laws increase healthcare prices and spending, which may be contributing to the medical debt crisis. See Noam N. Levey, “100 Million People in America Are Saddled with Health Care Debt,” KFF Health News, June 16, 2022.
[30]Al Dobson et al., An Evaluation of Illinois’ Certificate of Need Program (Springfield, IL: State of Illinois Commission on Government Forecasting and Accountability, February 2007).
[31]Thom Walsh, “Don’t Blame Medicare for Rising Medical Bills, Blame Monopolies,” Washington Monthly, June 19, 2023.
[32]Economists sometimes refer to this as the “Cadillac effect” because it assumes that consumers will prefer no service at all if they can’t have the very best service at hand.
[33]J. S. Zinn, “Market Competition and the Quality of Nursing Home Care,” Journal of Health Politics, Policy and Law 19, no. 3 (1994): 555–82.
[34]Thomas Stratmann, “The Effects of Certificate-of-Need Laws on the Quality of Hospital Medical Services,” Journal of Risk and Financial Management 15, no. 6 (2022): 272; Kevin Chiu, “The Impact of Certificate of Need Laws on Heart Attack Mortality: Evidence from County Borders,” Journal of Health Economics 79 (2021): 102518.
[35]Agnitra Roy Choudhury, Sriparna Ghosh, and Alicia Plemmons, “Certificate of Need Laws and Health Care Use during the COVID-19 Pandemic,” Journal of Risk and Financial Management 15, no. 2 (2022): 76.
[36]Zack Cooper et al., “The Price Ain’t Right? Hospital Prices and Health Spending on the Privately Insured” (NBER working paper no. 21815, National Bureau of Economic Research, Cambridge, MA, December 2015).
Certificate of Need Reform: Answering the Fears
- Answering the Fears
- Fear 1: Without CON Laws, Costs Will Rise as Hospitals Acquire Expensive and Unnecessary Equipment
- Fear 2: Without CON, Hospitals—Especially in Rural Areas—Will Disappear
- Fear 3: Without CON Laws, ASCs Will Pop Up and Take Away All the Most Profitable Services from Hospitals
- Fear 4: Without CON Laws, Quality Will Suffer Because CON Laws Lead to Fewer Providers, with Each Offering a Higher Volume of Care, and Higher Volume Leads to Greater Proficiency
- Fear 5: Healthcare Is Different: It Is Not a Free Market, So None of the Rules Apply
- Conclusion
